
{kind=link}

The financialization of health care started 2 generations back and is now in a run-to-fail feedback loop of insolvency.
Veteran readers know I have been important of U.S. healthcare for over a decade. When I use the term sickcare this is not a reflection on the hard work of frontline caretakers– it is a reflection of the financialization rewards that have actually misshaped the system’s top priorities and put it on a course to insolvency.
To describe how Health care became Sickcare, I’m sharing the viewpoint of an Expert. The financialization of health care started 2 generations back and is now in a run-to-fail feedback loop of insolvency. As I have frequently stated, Sickcare will bankrupt the country all by itself. Here is the Expert’s essay:
* * *
As your readers attempt to understand the American health system and its response to COVID, they might benefit from a short summary of the system’s present company model from someone on the inside.
It’s my hope that it will assist them make sense of what is going on around them.
I read, see, and hear others inside the system frightened for their incomes if they speak out and I repent of myself, as my income no longer depends upon my silence.
So I’m sharing this to speak for those who can’t.
For factors beyond the scope of this research study, and aside from a (extremely) couple of service lines, the delivery of healthcare is a low margin affair. Unless one keeps their overhead really low, revenue is difficult to achieve.
Yet, the consolidated health systems which progressively control the landscape are plainly high-overhead concerns, what with their staggering management bandwidth, shining palaces of recovery, and obscene executive payment.
How does one square this?
Health systems create profits from:
1. A (very) small number of profitable service lines, primarily plastics, some ortho, and a smattering of others.
2. Inflated book value of their commercial realty, often untaxed due to religious/not-for-profit status.
3. Bulk and private resale of patient information.
4. Kickbacks from suppliers, legal (purchase rebates) and illegal (direct payments).
5. Federal government grants.
Health systems don’t make their cash from the delivery of health care, they make their money by charging for the redirection of the firehose of third-party payments to which the shipment of healthcare grants them gain access to. This holds true for any health system which exceeds a particular fairly modest size and provides the majority of their care through third-party payers such as Medicare.
It holds true no matter their IRS classification; for-profit, not-for-profit, religious. The spiritual sponsored ones utilize their status as a religion to put themselves, politically and lawfully, at the best possible distance from internal revenue service examination.
Under this model, the company’s goal is merely to keep up the facade of providing healthcare at the most affordable possible expense and produce maximum income from all the secondary impacts.
Thank you Accountable Care Act.
For example, health systems:
1. Apparently collude with each other to keep clinicians and nurses salaries as low as possible
2. Make sure, if not favorable, a minimum of neutral media coverage through
a.The existence of media company management on their boards and vise-versa
b.Direct payment to those organizations either through overpriced marketing or direct rewards to their executives.
3. Emphasize the few profit-generating service lines, most recently COVID. Two years into the pandemic and for no genuine reason, COVID medical diagnoses still bring benefit compensation to the health systems. Making use of certain COVID-related meds carry “rebate” payments back to the systems.
4. decrease supply costs by either
a.Purchasing the vendors straight
b.Utilizing the most inexpensive supply chains whose quality is just enough to preserve the facade.
This last technique is why there was such a big shortage of PPE at the start of the pandemic. Supply chains reached into China where the least expensive alternatives were discovered. Sadly, those supply chains were fragile and dependence on them left couple of domestic suppliers able to ramp up deliveries.
This is also why there is such a great deal of “financializers” in executive positions. Their passion isn’t healthcare, it’s the access to the 20% of GDP the market grants them. When the pandemic hit, how many CEOs did you see in working in the ER for an hour approximately a week to show uniformity with the minimum wage staff members who, at unknown risk to themselves, were keeping the place running?
None. They were all in the 2nd homes in Florida. Their hearts remain in finance, not health care.
This worldview explains so many puzzling things.
Q. Why are bad conditions at hospitals not being reported?
A. Collusion with the media
Q. Why are hospitals able to let go of many employees, even in the middle of a pandemic?
A.They only need enough to service their couple of successful lines (COVID) while keeping up the appearance of delivering healthcare.
Q. Why is the capacity for the few profit-generating service lines, such as COVID ICU care, growing while it’s so challenging to get a visit for more ordinary services?
A.That’s where the cash is.
Q. Why are clinicians and nurses changing professions at an unmatched rate?
A.The current service design is incompatible with their personal objective of service. Guffaw if you like. Yes, they too like to earn money, however unlike the financial folks they must have an aspect of service in their vocation to be content. Otherwise, they also would have just entered into company. They are not able to square their individual mission with the commoditization of human life they are seeing.
So they leave.
Q. Why is the doctor suicide rate now the greatest among individuals with > 4 years college. At current development rates, soon 1/10000 doctors will kill themselves every year, an extraordinary number.
A.See above, then include financial obligation and disillusionment.
Consider this one of the fruits of delivering a subtle, subjective service such as health care through an assembly-line industrial model focused on making a dollar. The line employees and their training are mismatched to the task. Force petroleum wild-catters to sell Mary Kay and you’ll get the very same thing.
Q.Why do health systems continue to invest in commercial real estate?
A.They usage pre-pandemic foot traffic numbers to boost both the evaluations and the rental rates to occupants. Like in 2009, no one has an interest in marking the value of their investments to market.
Q. Why does everyone in health care invest so much time on the computer?
A. Since the data they’re gathering is a considerable source of income.
Q. Why does getting healthcare seem like such an assembly line?
A. Since that’s how the executives have actually been trained to keep down costs. They do not care about individual patients, they care about “patients” in aggregate for the factors detailed above.
Q. Why are health systems so dead set on getting their staff members the COVID shot?
A. “Rebates” from the supplier and ingratiating themselves to the political and regulatory classes who themselves are getting kickbacks also.
Q. Why are health systems emphasizing telemedicine?
A. Because they believe they can squeeze more productivity out of their companies while paying them the very same– it’s a method to reduce the costs related to keeping up the facade of delivering healthcare.
Is your health system among these? The much better their customer support, the less likely your health system follows this design.
This of course is an extension of Gresham’s Law; Bad Chases After Out Great, money initially, then everything else. When the currency is phony, it corrodes society itself. It is the tsunami of valueless fiat that makes keeps the whole edifice set up. The percentage of GDP we “spend” on “healthcare” in fact represents the percent of GDP that’s skimmed utilizing healthcare as a grift.
I think about the reader who operates under the presumption that health systems remain in business of providing healthcare.
They are actually in the business of, well, service.
And they’ve used their position to avoid any competition at scale. Fortunately, you and I don’t require healthcare at scale, we just need healthcare. So, look for a clinician who takes cash. Go to DPcare.org or take a look at the Surgical treatment Center of Oklahoma City. Cleveland Center will do your bypass for a flat cost, and pay for any problems. The rates are much less than one would anticipate, and you get excellent access to your personal clinician, not as one of 5000 patients, but as one of 500.
We must eliminate ourselves of the idea that our Medicare and medical insurance premiums pay for health care. They’re simply taxes for which we’ll acquire restricted worth, at best they represent devastating coverage. To get important health care, we are going to have to pay for it ourselves.
I don’t represent, personally supply, or have any monetary interest in cash-pay healthcare.
As resources decline and health systems focus progressively on the grift instead of care, direct payment for health care will continue to grow under the radar– as it doesn’t (yet) threated the health systems’ position.
Compared to expectations, cash-pay is surprisingly affordable, the care experience is better, and it includes really little valueless, harmful, or excess care.
It is my hope that the worldview above helps your readers explain and perhaps predict the behavior of these health systems going forward.
* * *
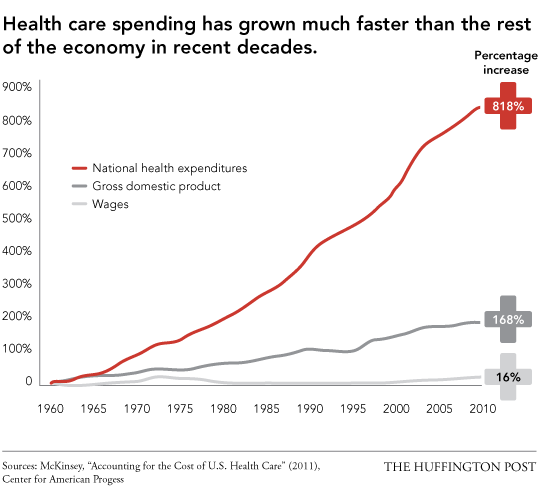
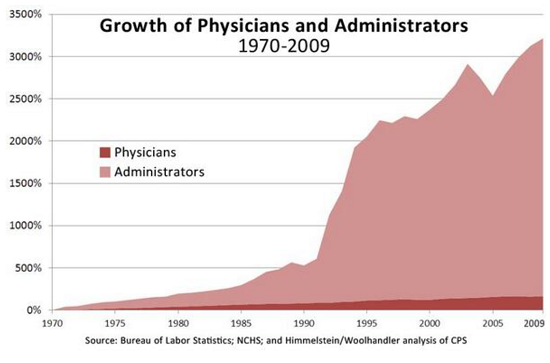
Thank you, Insider. As I have actually have noted lot of times, if you still believe that America’s system is “the finest in the world” and is endlessly sustainable, please research study these three charts and extend the trendlines.
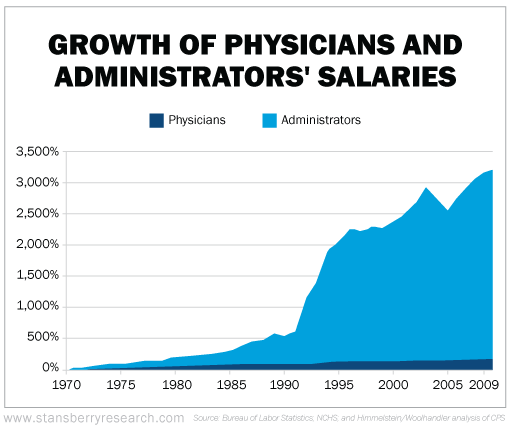
< img align="center"src= "https://www.oftwominds.com/photos2020/doctors-administrators-salaries.png"width="550"/ > My new book is now offered at a 10 % discount this month: Global Crisis, National Renewal: A(Revolutionary)Grand Method for the United States(Kindle$8.95, print$20)If you found value in this content, please join me in looking for services by becoming a$1/month customer of my work through patreon.com. Recent Videos/Podcasts: Charles Hugh Smith on The Great
Awakening Vision(Part II, 36 minutes, with Richard Bonugli)Charles Hugh Smith on The Great Reset Agenda(Part I, 42 minutes, with Richard Bonugli)My recent books: Global Crisis, National Renewal: A(Revolutionary)
Grand Method for the United States(
?: Earnings, Power, and AI in a Traumatized World(Kindle$5, print$10, audiobook)Check out the very first area for free(PDF). Pathfinding our Fate: Preventing the Final Fall of Our Democratic Republic($5 Kindle,$10 print, (audiobook): Check out the first section for
totally free(PDF). The Adventures of the Consulting Theorist: The Disappearance of Drake $1.29 Kindle, $8.95 print ); checked out the very first chapters totally free(PDF)Cash and Work Unchained$6.95 Kindle,$ 15 print) Check out the very first section free of charge End up being
a$1/month client of my work by means of patreon.com. NOTE: Contributions/subscriptions are acknowledged in the order received. Your name and e-mail stay personal and will not begiven to any other specific, company or agency. Thank you, David M.($100), for your outrageously generous contribution to this website– I am significantly honored by your assistance and readership. Thank you, Laura D.($50), for your magnificently generous contribution to this website– I am considerably honored by your unfaltering support and readership. Thank you, William C. ( $50), for your monstrously generous contribution to this site– I am considerably honored by your steadfast support and readership. Thank you, Chad D.($50), for your marvelously generous contribution to this site– I am considerably honored by your unfaltering support and readership.